

ADVERTISEMENT
Successful Treatment of a Late Presentation Exercise-Induced Spontaneous Left Anterior Descending Artery Dissection
ABSTRACT: Spontaneous coronary artery dissection is an unusual condition that mainly happens in fit and healthy women in the peripartum period. Strenuous exercise is a rare cause of dissection in angiographically normal coronary arteries. There is no definitive consensus on the aetiology, prognosis and treatment of SCAD. We report a case of successful treatment of a late presentation of a coronary artery dissection secondary to intense physical activity in a 48 year old cyclist who continued to cycle for 3 months post event.
J INVASIVE CARDIOL 2011;23(11):E260-E262
Key words: coronary intervention, IVUS, SCAD
____________________________________
Spontaneous coronary artery dissection (SCAD) is an increasingly recognized condition that can lead to acute coronary syndromes and often affects younger people. Its diagnosis has been made easier by modern imaging techniques such as coronary angiography. Here we consider the management of a patient with a more chronic presentation.
Case Report. A 48-year-old female patient presented to Rapid Access Chest Pain clinic in a district general hospital complaining of exertional chest tightness (manifesting as a central, heavy sensation) and dyspnea since a cycling tour in South Africa four months previously. The patient had experienced a sudden onset of sharp central chest pain whilst negotiating a steep incline. It did not radiate but both increased with progressive exertion and was associated with dyspnea. The symptoms resolved with rest and following this short break, she was able to continue, albeit at a reduced workload. The patient reported no significant past medical history and she was not taking any medication. She denied any risk factors for ischemic heart disease (although her total cholesterol level on the presentation day was 5.9mmol/L). Clinical examination was unremarkable. No evidence of connective tissue disease was detected. The 12 lead electrocardiogram (ECG) showed T wave inversion across the anteroseptal leads. It was felt that the history was of classical angina and that given the distribution of the ECG changes and hyperlipidemia the patient had a moderate risk of coronary artery disease and warranted coronary angiography.
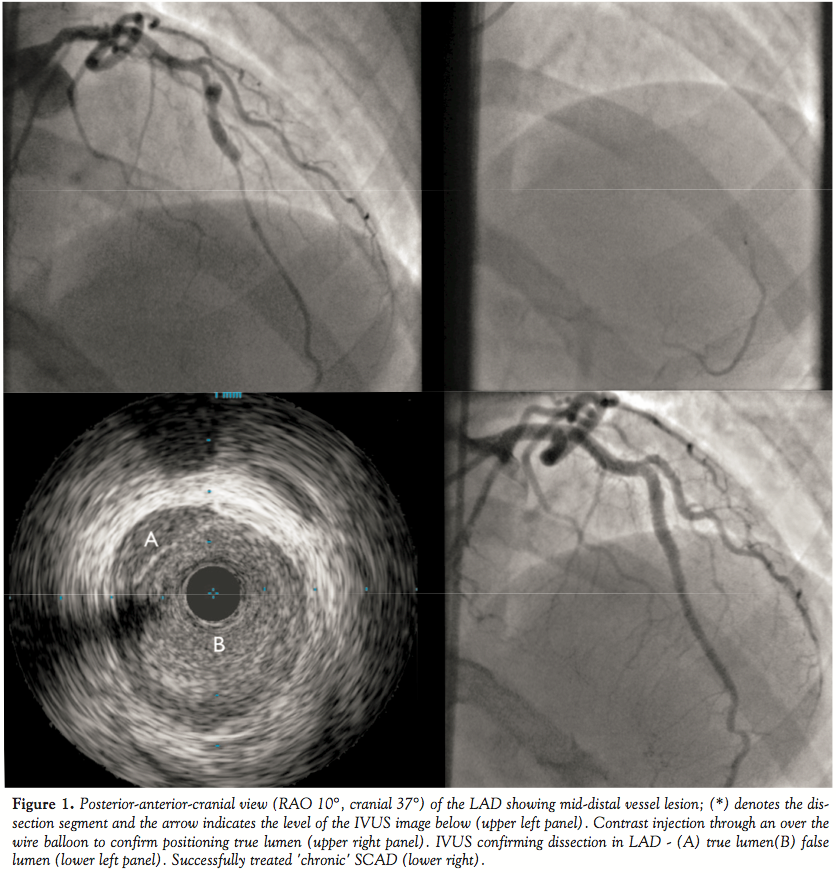 Cardiac catheterization was performed via the right femoral artery and demonstrated unobstructed left main stem (LMS), circumflex and right coronary arteries (RCA). However there was a flow-limiting lesion in the mid left anterior descending (LAD) (Figure 1). She was referred to a tertiary cardiology center for further assessment of, and possible intervention to this lesion. The patient received aspirin 300 milligrams (mg) and clopidogrel 600mg pre-loading. Further catheterization was performed via the right femoral artery using a 6 Fr sheath. The LMS was intubated using a JL 3.5 guide catheter and selective coronary angiography revealed a likely dissection flap in the mid-LAD (Figure 1). The lesion was crossed carefully with a floppy-tipped 0.016" Luge wire (Boston Scientific Corp.). To confirm position within the true lumen a Ryujin Plus over-the-wire balloon was passed distal to the lesion and injection of contrast demonstrated filling of the distal LAD (Figure 1). The dissection was confirmed on intravascular ultrasound (IVUS) using a Volcano Revolution rotational IVUS catheter (Volcano Corp.) (Figure 1). The distal end of the dissection flap was stented using a 2.75 x 28 mm Xience PRIME SV everolimus-eluting stent (Abbot Vascular), post-dilated using a 3.5 x 12mm Quantum non-compliant balloon (Boston Scientific). This was overlapped proximally with an additional 3.5 x 18mm Xience PRIME SV stent. The overlapping portion and proximal stents were post-dilated using a 4 x 12mm Quantum balloon. Full and even deployment of the stents was verified using IVUS as before, also confirming resolution of the dissection flap with a good final angiographic appearance (Figure 1). The patient was prescribed maintenance dual anti-platelet therapy of aspirin 75mg od and clopidogrel 75mg OD for a minimum of twelve months. She also received secondary prevention in the form of Atorvastatin 40mg OD and Atenolol 25mg OD.
Cardiac catheterization was performed via the right femoral artery and demonstrated unobstructed left main stem (LMS), circumflex and right coronary arteries (RCA). However there was a flow-limiting lesion in the mid left anterior descending (LAD) (Figure 1). She was referred to a tertiary cardiology center for further assessment of, and possible intervention to this lesion. The patient received aspirin 300 milligrams (mg) and clopidogrel 600mg pre-loading. Further catheterization was performed via the right femoral artery using a 6 Fr sheath. The LMS was intubated using a JL 3.5 guide catheter and selective coronary angiography revealed a likely dissection flap in the mid-LAD (Figure 1). The lesion was crossed carefully with a floppy-tipped 0.016" Luge wire (Boston Scientific Corp.). To confirm position within the true lumen a Ryujin Plus over-the-wire balloon was passed distal to the lesion and injection of contrast demonstrated filling of the distal LAD (Figure 1). The dissection was confirmed on intravascular ultrasound (IVUS) using a Volcano Revolution rotational IVUS catheter (Volcano Corp.) (Figure 1). The distal end of the dissection flap was stented using a 2.75 x 28 mm Xience PRIME SV everolimus-eluting stent (Abbot Vascular), post-dilated using a 3.5 x 12mm Quantum non-compliant balloon (Boston Scientific). This was overlapped proximally with an additional 3.5 x 18mm Xience PRIME SV stent. The overlapping portion and proximal stents were post-dilated using a 4 x 12mm Quantum balloon. Full and even deployment of the stents was verified using IVUS as before, also confirming resolution of the dissection flap with a good final angiographic appearance (Figure 1). The patient was prescribed maintenance dual anti-platelet therapy of aspirin 75mg od and clopidogrel 75mg OD for a minimum of twelve months. She also received secondary prevention in the form of Atorvastatin 40mg OD and Atenolol 25mg OD.
At one month follow-up the patient complained of atypical chest pain and underwent exercise tolerance testing according to the Bruce protocol for 15 minutes and 30 seconds achieving 17.90 METS and 95% of her maximum predicted heart rate without symptoms nor ECG changes. She has now returned to full activities and resumed heavy exercise again without any further complaint of chest pain or shortness of breath.
Discussion. In contrast to traumatic coronary dissection, such as due to blunt chest trauma or iatrogenic dissection during coronary angiography, PCI or cardiac surgery, primary spontaneous coronary artery dissection (SCAD) is an unusual cause of acute coronary syndrome (ACS). Its incidence is markedly less frequent than aortic dissection. It was originally described in 1931 following a post-mortem examination of a 42-year-old woman who died suddenly.1 The first angiographic report was published in 1978.5 The defect is a separation of the layers of the coronary artery wall. In patients without underlying atherosclerosis this usually occurs between the media and adventitia. Subsequent hematoma formation within the false lumen compresses the true lumen leading to impaired coronary artery flow, myocardial oxygen demand/supply mismatch and ischemia.
A literature review shows more than 300 cases have been published since 1931.2,3,7 The age range at presentation is usually 30 to 45 years and more than 70% of cases are seen in women.2,8,9 The most common presentation is that of a peripartum episode in otherwise fit and healthy women who have no coronary atherosclerosis. Other causes include connective tissue disorders (such as type IV Ehlers-Danlos syndrome or Marfan’s syndrome), vasculitis, cocaine abuse, prolonged sneezing, contraceptive pills and idiopathic dissection.2 True and spontaneous dissection of non-atherosclerotic coronary arteries occurring during intense activity is less common. Intense physical activity could cause acute plaque rupture in an atherosclerotic artery, but whether this is truly SCAD is debatable.4 In women, dissection in the LAD is most frequent whereas in men the RCA is most commonly involved1 — dissection of the LMS is rare.10 Clinical presentation can range from asymptomatic patients with ECG changes to sudden cardiac death.2,11 It seems likely that our patient suffered an ACS at the index event during peak exercise, and the delay in presentation is unusual given that some estimate the mortality to be as high as 70%.12
The typical appearance of a coronary artery dissection on coronary angiography is the presence of a thin longitudinal radiolucent line representing the dissection flap with flow in two or more separate lumens.2 However, diagnosis by angiography alone is difficult: occasionally the absence of an obvious flap can lead to interpretation of the defect as a long eccentric plaque.2 Unless the appearance is very clear on conventional angiography, intra-coronary imaging with IVUS can be extremely helpful in both making the diagnosis and guiding management, as shown in this case.
There are only limited data on the optimal treatment strategy. The use of antiplatelets and heparin may limit clot/hematoma formation and its associated flow limitation.13 The mechanical effects of the compression or further extension of the dissection flap could be limited by nitrates, beta-blockade or calcium channel blockers.14 As demonstrated in our case, percutaneous coronary intervention (PCI) is possible even in long segments of established dissection. The key to PCI in these cases is ensuring that one operates within the true lumen of the vessel — in this case we utilized an over-the-wire balloon to demonstrate filling of the distal vessel with contrast injection.
Conclusion. SCAD is an important diagnosis in seemingly low-risk individuals for ischemic heart disease. It is important to recognize it as a differential in presentations of chest pain. Successful PCI can be achieved even in markedly delayed presentations to return individuals to normal function.
References
- Pretty HC. Dissecting aneurysm of coronary in a woman aged 42. BMJ. 1931;1: 667.
- Vrints CM. Spontaneous coronary artery dissection. Heart. 2010;96(10):801-808.
- Atay Y, Yağdi T, Türkoğlu C, Altintiğ A, Büket S. Spontaneous dissection of left main coronary artery: review of literature. J Card Surg. 1996;11(5):371-375.
- Kalaga RV, Malik A, Thompson PD. Exercise- related spontaneous coronary artery dissection. Med Sci Sports Exerc. 2007;39(8):1218-1220.
- Ciraulo DA, Chesne RB. Coronary Arterial Dissection and unrecognised cause of myocardial infarction, with subsequent coronary arterial patency. Chest. 1978;73(5): 677-679.
- Sharma AD, Sreeram G, Slaughter TF. Spontaneous coronary artery dissection in a healthy 24-year old woman. J Cardiovascular Anaesthesia. 2000;14(3):312-313.
- Corrado D, Thiene G, Cocco P, Frescura C. Non-atherosclerotic coronary artery disease and sudden death in the young . Heart. 1992;68(6):601-607.
- DeMaio SJ Jr, Kinsella SH, Silverman ME. Clinical course and long-term prognosis of spontaneous coronary artery dissection. Am J Cardiology. 1989;64(8):471-474.
- Thompson EA, Ferrraris S, Gress T, et al. Gender differences an predictors of mortality in spontaneous coronary artery dissection: a review of reported cases. J Invasive Cardiol. 2005;17(1):59-61.
- Verma PK, Sandhu MS, Mittal BR, Aggarwal N, Kumar A, Mayank M, et al. Large spontaneous coronary artery dissections: a study of three cases, literature review and possible therapeutic strategies. Angiology. 2004;55(3):309-318.
- Hering D, Piper C, Hohmann C, Schultheiss HP, Horstkotte D. Prospective study of the incidence, pathogenesis and therapy of spontaneous, by coronary angiography diagnosed coronary artery dissection (article in German). Z Kardiol. 1998;87(12):961-970.
- Cocco P, Thiene G, Corrado D, Lodovichetti G, Pennelli N. Ematoma (aneurysm) dissecante spontaneo delle coronary e more improvivisa. G Ital Cardiol. 1990;20(9):795-800.
- Sarmento-Leite R, Machado PR, Garcia SL. Spontaneous coronary artery dissection: stent or wait for healing? Heart 2003;89(2):164-166.
- Choi JW, Davidson CJ. Spontaneous multivessel coronary artery dissection in a long-distance runner successfully treated with oral antiplatelet therapy. J Invasive Cardiol 2002;14(11):675-678.
____________________________________
From the 1Kingston Hospital, Galsworthy Road, Kingston upon Thames, Surrey, KT2 7QB, United Kingdom, 2King’s College London, BHF Centre of Excellence, Cardiovascular Division, St Thomas’ Hospital, London, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. No conflicts of interest were reported regarding the content herein.
Manuscript submitted March 21, 2011, provisional acceptance given April 14, 2011, final version accepted August 4, 2011.
Address for correspondence: Shana Tehrani, MD MRCP ª, Kingston Hospital, Galsworthy Road, Kingston upon Thames, Surrey, KT2 7QB, United Kingdom. Email: s.tehrani@ucl.ac.uk

