

ADVERTISEMENT
The Spontaneous Coronary Slow-Flow Phenomenon: Reversal by Intracoronary Nicardipine
Abstract
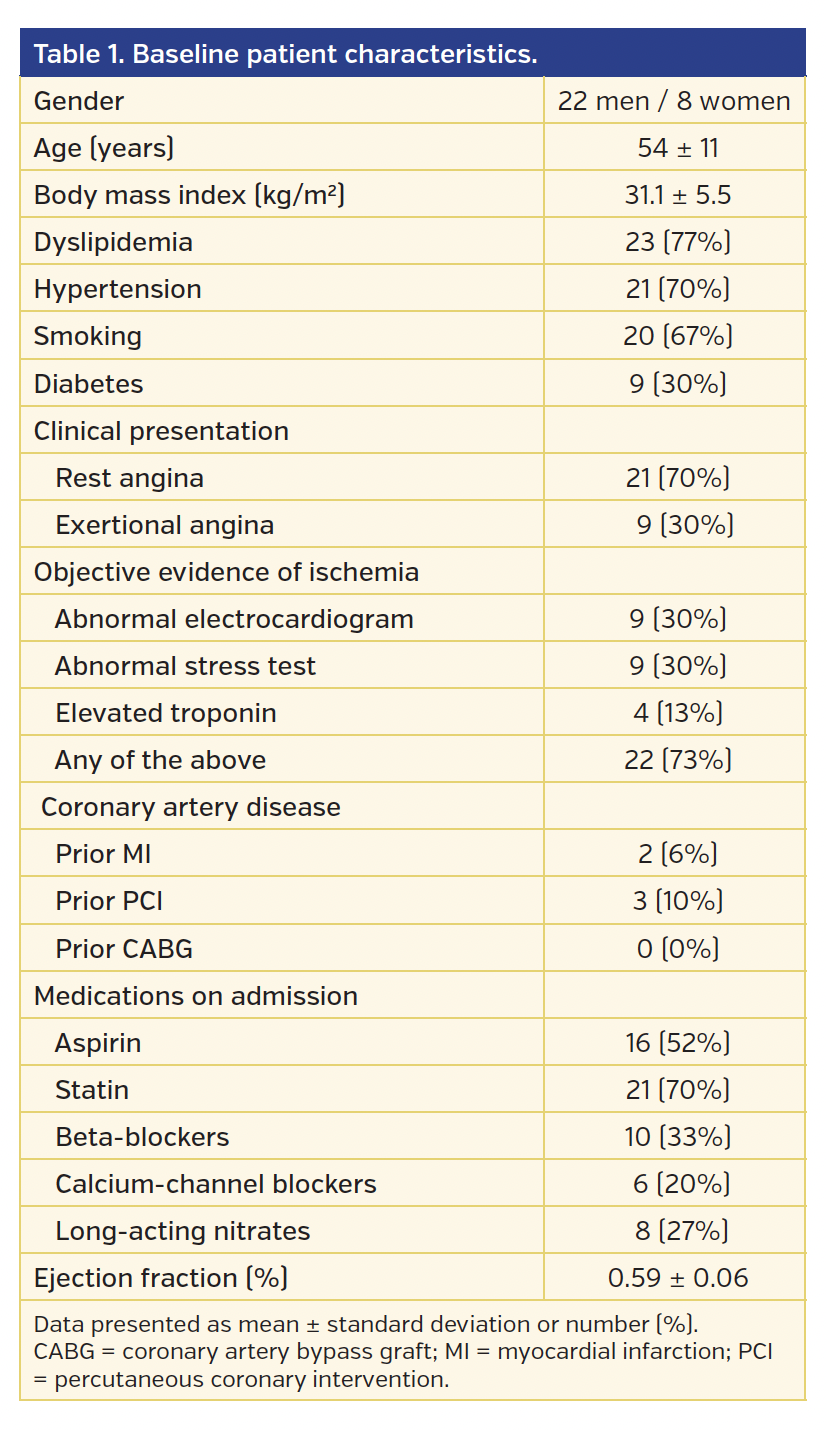
Abstract: Objective. An under-recognized cause of chest pain, the coronary slow-flow (CSF) phenomenon is characterized by delayed coronary opacification during diagnostic angiography in the absence of epicardial coronary artery disease (CAD). Given its angiographic resemblance to no-reflow during percutaneous coronary intervention, a condition associated with microvascular spasm responsive to calcium-channel blockers, we hypothesized that spontaneous CSF may similarly be reversed by intracoronary (IC) nicardipine. Methods. The effect of IC nicardipine was evaluated in 30 patients. CSF was defined as spontaneously delayed flow (<TIMI 3) during diagnostic coronary angiography in the absence of obstructive epicardial CAD or other conditions associated with impaired flow. Nicardipine was administered as a 200 µg IC bolus, after which repeat angiography was performed. Coronary flow before and after nicardipine was evaluated by TIMI flow grade and corrected TIMI frame count (TFC) assessments. Results. The study population consisted of 22 men and 8 women (mean age, 54 ± 11 years). Clinical presentation was rest angina in 21 patients (70%). At baseline, CSF with <TIMI 3 flow was observed in 49 vessels. TFC was prolonged (>27) in 68/90 vessels (76%). IC nicardipine produced markedly accelerated coronary filling, which was corroborated by TFC analysis. TFC was 47 ± 17 before vs 15 ± 5 after nicardipine (P<.001). All vessels demonstrated TIMI 3 flow and TFC <28 after nicardipine treatment. Conclusions. IC nicardipine appears highly effective in reversing spontaneous CSF. These findings implicate microvascular spasm in the pathogenesis of CSF. Future studies of oral calcium-channel blockers in the long-term management of CSF are needed.
J INVASIVE CARDIOL 2019;31(3):42-45. Epub 2018 December 15.
Key words: coronary microcirculation, coronary slow flow phenomenon, acute coronary syndromes, microvascular spasm
Introduction
Chest pain contributes to frequent emergency room visits and is a leading cause of increasing health-care costs. An under-recognized cause of chest pain, the coronary slow flow (CSF) phenomenon is characterized by delayed coronary opacification during diagnostic angiography in the absence of obstructive epicardial coronary artery disease (CAD) or other conditions that are known to impair coronary flow.1,2 First described in 1972, CSF may be more common than generally appreciated. CSF has been described in up to 7% of patients undergoing diagnostic angiography and may account for up to 4% of unstable angina admissions.1,3 The clinical course can be challenging, with recurrence of chest pain occurring in up to 80% of patients and hospital readmission in 20% within a 2-year follow-up period.4 While the pathophysiology of CSF is not fully understood, abnormally elevated microvascular resistance appears to be an important feature.5 Because of the angiographic similarity of CSF to no-reflow observed during percutaneous coronary intervention (PCI) – a condition associated with microvascular spasm – we hypothesized that CSF may be reversed by intracoronary (IC) administration of nicardipine. Nicardipine, a dihydropyridine calcium-channel blocker with selective vasodilatory effects, has been shown to increase coronary blood flow and reverse no-reflow complicating PCI.6-9 Accordingly, the goal of this study was to assess the effect of IC nicardipine on the CSF phenomenon.
Methods
The effect of IC nicardipine on CSF was assessed in 30 patients. CSF was defined as the presence of angiographically normal or near-normal coronary arteries and Thrombolysis in Myocardial Infarction (TIMI) 2 flow (requiring >3 beats to opacify prespecified branch points in the distal vasculature of at least one of the three major epicardial coronary vessels).1,3 Patients were excluded if there were coronary artery stenoses >40% or other conditions that can be associated with impaired coronary flow (recent PCI, coronary artery ectasia, epicardial coronary arterial spasm, cardiomyopathy, or significant valvular heart disease).
Nicardipine was prepared in a diluted solution of normal saline with a concentration of 100 µg/1 mL. Nicardipine was administered as a 200 µg intracoronary bolus, after which repeat angiography was performed. Coronary flow before and after nicardipine was assessed by TIMI flow grade and by the corrected TIMI frame count (TFC) based on previously established criteria by Gibson et al.10 TIMI flow grade <3 and TFC ≥28 were considered abnormal.
Demographic data are reported as mean ± standard deviation or number (percentage). Differences in TFC before and after IC nicardipine were evaluated by paired t-tests. A P-value <.05 was considered statistically significant. This retrospective study was approved by the Institutional Review Board of the participating hospitals.
Results
Demographic characteristics of the study cohort are detailed in Table 1. The patient population consisted of 22 men and 8 women with a mean age of 54 ± 11 years (range, 28 to 79 years). The majority of patients (70%) presented with rest angina. Cardiovascular risk factors included dyslipidemia in 23 patients (77%), hypertension in 21 patients (70%), tobacco use in 20 patients (67%), and diabetes in 9 patients (30%). Objective evidence of ischemia was demonstrated in 18 patients (60%) by abnormal electrocardiogram or stress testing; elevated troponin T level was present in 4 patients (13%).

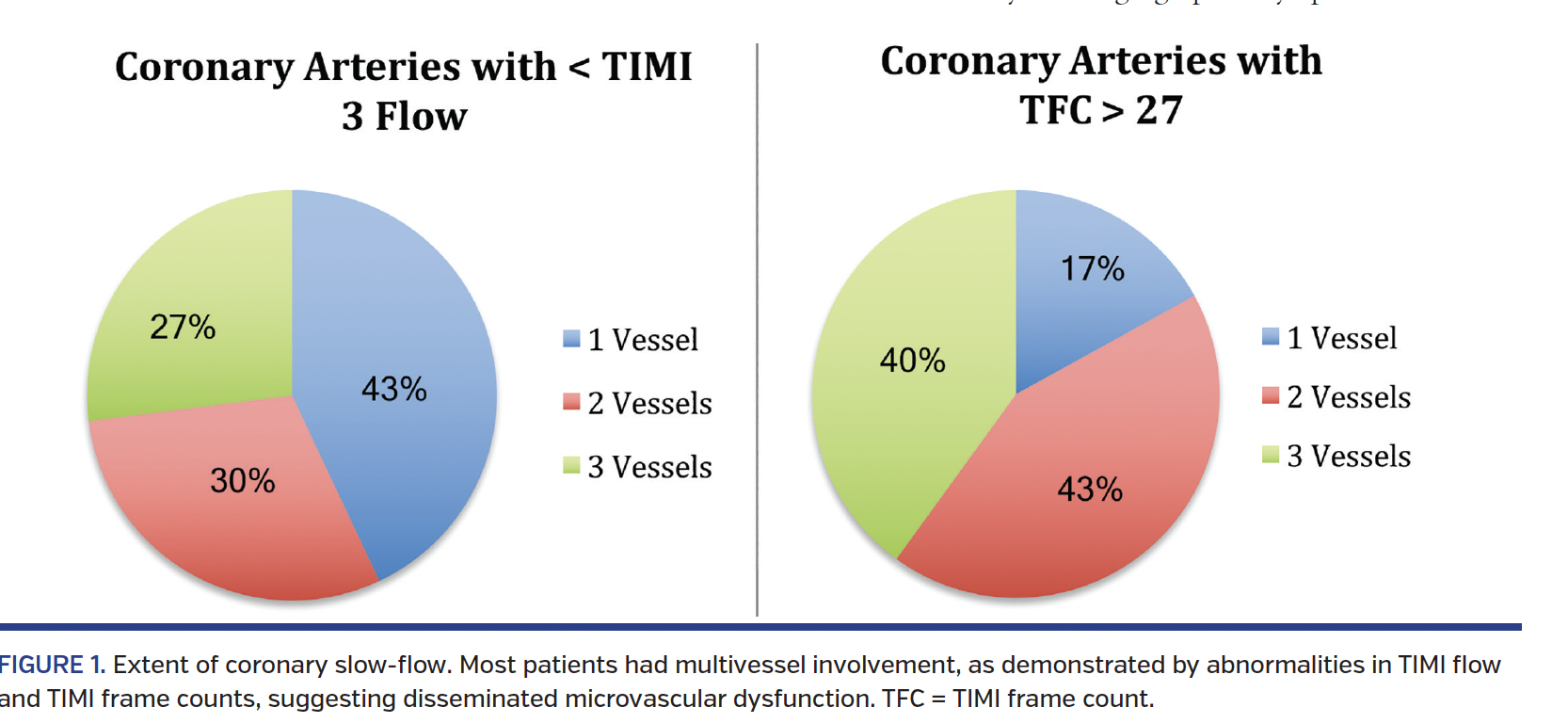
At baseline, CSF (TIMI flow <3) was observed in 49 epicardial coronary arteries. Multivessel involvement was present in 57% (Figure 1). The presence of CSF by vascular distribution was as follows: left anterior descending, 28 (93%); left circumflex, 7 (23%); and right coronary artery, 14 (47%). Prolonged TFC was present in 68 of 90 epicardial vessels (76%), suggesting disseminated microvascular dysfunction in CSF.

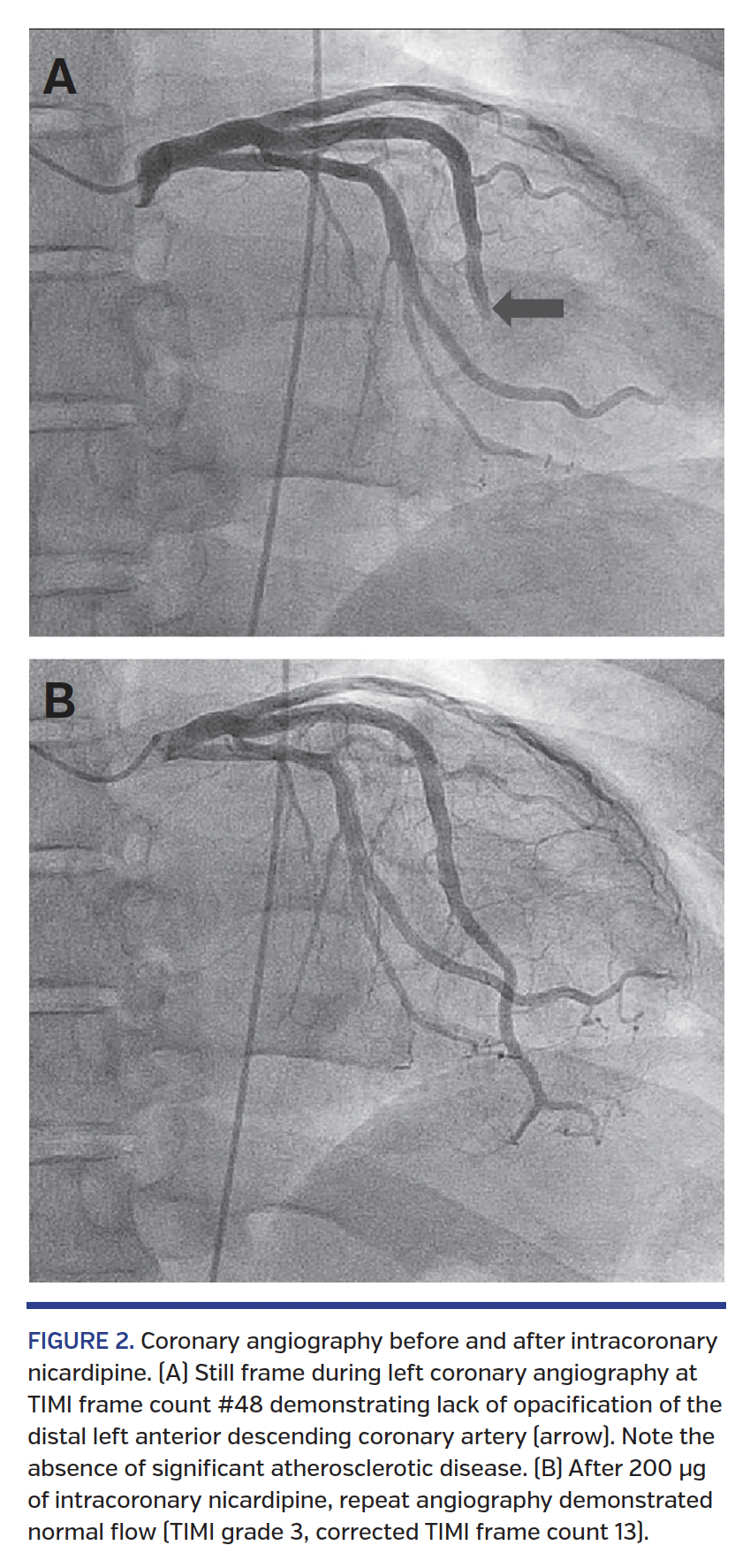
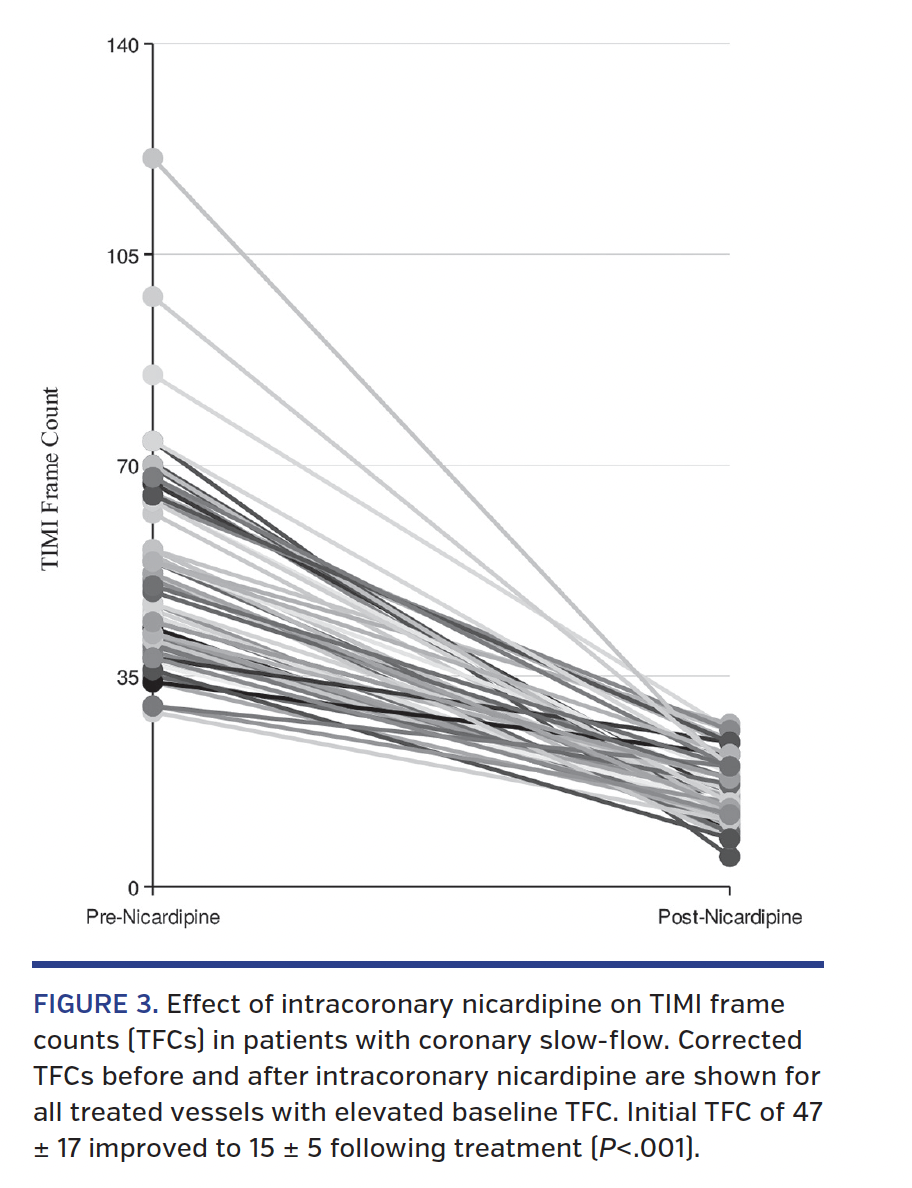
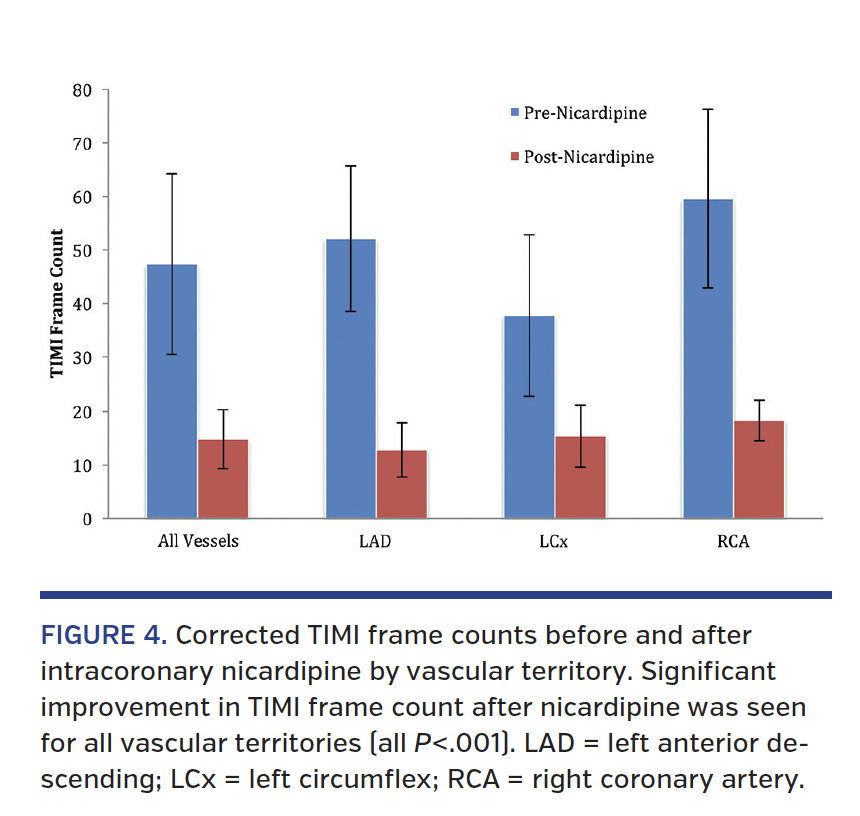
IC nicardipine characteristically resulted in markedly accelerated angiographic filling of the coronary arteries (Figure 2; Video 1); this observation was corroborated by TIMI flow and TFC analysis. In vessels with CSF, TFC improved from 47 ± 17 at baseline to 15 ± 5 after IC nicardipine administration (P<.001) (Figure 3). All vessels demonstrated TIMI 3 flow and TFC <28 following nicardipine. Significant improvement in TFC was seen for all vascular territories (Figure 4). No adverse effects were observed with drug administration.



Discussion
As previous studies have described, not all microvascular flow abnormalities are equal.2 While microvascular dysfunction is also seen in classic coronary syndrome X, CSF (also labeled as “syndrome Y”) has been previously described to be a distinct entity.11,12 Angiographically spontaneous CSF resembles the appearance of the no-reflow phenomenon, which occurs during PCI. Since the latter condition is associated with microvascular spasm, which is responsive to IC calcium-channel blockers, we hypothesized that spontaneous CSF might be similarly reversed by administration of IC nicardipine. Use of IC nicardipine has been reported to be effective in the treatment and prevention of no-reflow during PCI.8,9,20 In the current study, nicardipine was found to be highly effective in reversing spontaneous CSF, as demonstrated by an increase in TIMI flow and a reduction in TFC following IC administration. These findings implicate microvascular spasm in the pathogenesis of the CSF phenomenon.
CSF patients are commonly young male smokers who present with rest angina with ischemia on resting electrocardiogram and normal stress test, as opposed to postmenopausal females with exertional angina and ischemia on stress testing typically seen in syndrome X.4,13 Previous authors have suggested that CSF may possibly be a cause of MI and even sudden cardiac death in patients with otherwise normal coronaries.14-19 Although ischemia is not commonly demonstrated on stress imaging, its presence appears to identify patients with CSF who are at increased risk of adverse outcomes.14,15 Recurrent episodes of chest pain and hospital readmission are common.4
Increased coronary microvascular resistance appears to be integral to the mechanism of CSF. Fineschi et al demonstrated that in patients with CSF, microvascular resistance was increased and CFR was decreased under basal resting conditions.5 These abnormalities were shown to be reversible following administration of IC papaverine. Thus, CFR was preserved in CSF despite the significant elevation in resting microvasculature resistance. These findings in CSF stand in contrast to syndrome X, where CFR is impaired. The preserved vascular response to vasodilators such as papaverine, dipyridamole, and adenosine, which improve the high microvascular resistance, is a distinguishing feature that differentiates CSF from syndrome X.11 Nicardipine is a dihydropyridine calcium-channel blocker with selective vasodilatory effects.6 IC administration of nicardipine has been shown to result in more potent and prolonged increase in coronary blood flow compared to verapamil and diltiazem;7 these favorable pharmacologic attributes and the established efficacy in the management of iatrogenic no-reflow were the basis for use of nicardipine in this study.
Study limitations. The limitations of this study are its retrospective nature and the relatively small number of patients. While IC nicardipine had a consistent, rapid impact on CSF, the duration of effect remains unknown. In addition, the role of oral calcium-channel blockers in long-term therapy is yet to be determined.
Conclusion
Administration of IC nicardipine appears highly effective in reversing the spontaneous CSF phenomenon. These findings implicate microvascular spasm in the pathogenesis of CSF and have potential therapeutic ramifications. Further studies of oral dihydropyridine calcium-channel blockers in the treatment of CSF are needed.
Affiliations and Disclosures
From 1Thomas Jefferson University Hospital, Philadelphia, Pennsylvania; 2University of Cincinnati Medical Center, Cincinnati, Ohio; and 3Our Lady of Lourdes Medical Center, Camden, New Jersey.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted October 8, 2018, provisional acceptance given October 15, 2018, final version accepted October 23, 2018.
Address for correspondence: Michael P. Savage, MD, Cardiac Catheterization Laboratory, Thomas Jefferson University Hospital, 111 South 11th Street, Gibbon Building, Ste 6210, Philadelphia, PA 19107. Email: michael.savage@jefferson.edu Twitter: @DocSavageTJU
References
1. Tambe AA, Demany MA, Zimmerman HA, Mascarenhas E. Angina pectoris and slow flow velocity of dye in coronary arteries. A new angiographic finding. Am Heart J. 1972;84:66-71.
2. Finley JJ, Savage MP. Coronary slow flow phenomenon: more than just an angiographic curiosity. Interv Cardiol. 2012;4:337-347.
3. Mangieri E, Macchiarelli G, Ciavolella M, et al. Slow coronary flow: clinical and histopathological features in patients with otherwise normal epicardial coronary arteries. Cathet Cardiovasc Diagn. 1996;37:375-381.
4. Beltrame JF, Limaye SB, Horoqitz JD. The coronary slow flow phenomenon—a new coronary microvascular disorder. Cardiology. 2002;97:197-202.
5. Fineschi M, Bravi A, Gori T. The “slow coronary flow” phenomenon: evidence of preserved coronary flow reserve despite increased resting microvascular resistance. Int J Cardiol. 2008;127:358-361.
6. Lambert CR, Pepine CJ. Effects of intravenous and intracoronary nicardipine. Am J Cardiol. 1989;64:8H-15H.
7. Fugit MD, Rubal BJ, Donovan DJ. Effects of intracoronary nicardipine, diltiazem, and verapamil on coronary blood flow. J Invasive Cardiol. 2000;12:80-85.
8. Fischell TA, Maheshwari A. Current applications for nicardipine in invasive and interventional cardiology. J Invasive Cardiol. 2004;16:428-432.
9. Huang RI, Patel P, Walinsky P, et al. Efficacy of intracoronary nicardipine in the treatment of no-reflow during percutaneous coronary intervention. Catheter Cardiovasc Interv. 2006;68:671-676.
10. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996;93:879-888.
11. Leone MC, Gori T, Fineschi M. The coronary slow flow phenomenon: a new cardiac “Y” syndrome? Clin Hemorheol Microcirc. 2008;39:185-190.
12. Gori T, Fineschi M. Two coronary “orphan” diseases in search of clinical consideration: coronary syndromes X and Y. Cardiovasc Ther. 2012;30:e58-e65.
13. Lanza GA, Crea F. Primary coronary microvascular dysfunction: clinical presentation, pathophysiology, and management. Circulation. 2010;121:2317-2325.
14. Yetkin E, Turhan H, Erbay AR, et al. Increased thrombolysis in myocardial infarction frame count in patients with myocardial infarction frame count in patients with myocardial infarction and normal coronary arteriogram: a possible link between slow coronary flow and myocardial infarction. Atherosclerosis. 2005;81:193-199.
15. Kapoor A, Goel PK, Gupta S. Slow coronary flow – a cause for angina with ST segment elevation and normal coronary arteries. A case report. Int J Cardiol. 1998;67:257-261.
16. Celik T, Ivyisoy A, Kursaklioglu H, et al. ST elevation during treadmill exercise test in a young patient with slow coronary flow: a compared with report and review of literature. Int J Cardiol. 2006;112:e1-e4.
17. Tatli E, Yildirim T, Aktoz M. Does coronary slow flow phenomenon lead to myocardial ischemia? Int J Cardiol. 2009:131:e101-e102.
18. Saya S, Hennebry TA, Lozano P, et al. Coronary slow flow phenomenon and risk for sudden cardiac death due to ventricular arrhythmias: a case report and review of the literature. Clin Cardiol. 2008;31:352-355 .
19. Amasyali B, Turhan H, Kose S, et al. Aborted sudden cardiac death in a 20-year-old man with slow coronary flow. Int J Cardiol. 2006;109:427-429.
20. Fischell T, Subraya R, Ashraf K, Perry B, Haller S. “Pharmacologic” distal protection using prophylactic, intragraft nicardipine to prevent no-reflow and non-Q-wave myocardial infarction during elective saphenous vein graft intervention. J Invasive Cardiol. 2007;19:58-62.

